Electrical impedance tomography (EIT) is a radiation-free, non-invasive imaging technique that uses measurements from surface electrodes to create a tomographic image of the body. EIT is particularly suited to assessing lung function: while conventional radiological imaging reveals lung morphology, EIT can be used to directly monitor regional lung ventilation and perfusion, and track changes due to disease or therapy.
To date, however, few EIT studies have examined the respiratory differences between men and women. To address this shortfall, a team from the University Medical Centre Schleswig-Holstein in Kiel, Germany has performed a detailed study of large group of volunteers to investigate how biological sex affects EIT measurements. Their findings suggest that key differences exist, and that these must be considered when interpreting clinical chest EIT studies.
“The anatomical and physiological differences between women and men make it important to determine sex differences in medical research,” explains first author Inéz Frerichs. “The relative lack of studies on sex-dependent differences in EIT findings is related to the fact that the method is not so old and large population studies in this field still need to be conducted. Small pilot studies do not have the power to establish possible differences reliably.”
Detailed data analysis
EIT works by applying small alternating currents through pairs of electrodes attached to the skin near the organ being examined. Measuring the resulting voltage differences through all adjacent electrode pairs enables construction of a 2D tomographic map of the electrical conductivity of that body part.
In their latest study, described in Physiological Measurement, Frerichs and colleagues analysed data from 218 adults with no known lung disorders who had participated in a previous EIT study. The cohort included 120 men and 98 women, with no significant differences between the subgroups asides height and weight. The team examined EIT recordings obtained during about one minute of quiet relaxed breathing (known as tidal breathing), with the subject seated.
The EIT exams were performed using an array of 16 electrodes placed around the lower chest, with the reference electrode attached onto the belly. Data were acquired at a rate of 33 images/s – a high scan rate that allows continuous assessment of dynamic physiological processes.
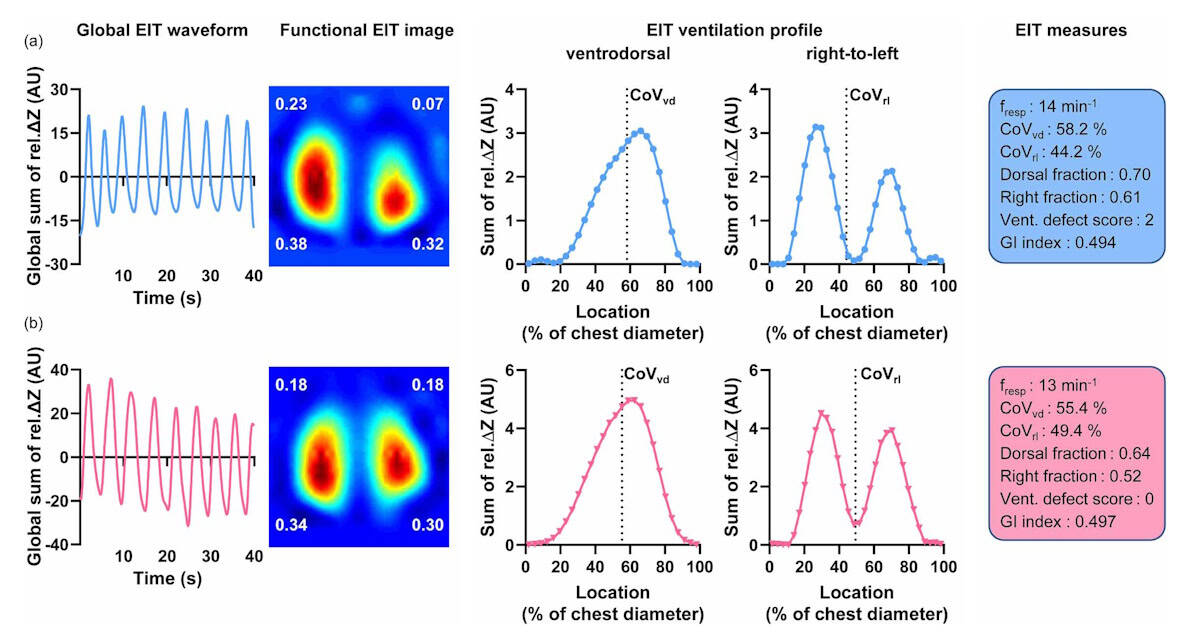
For all subjects, the researchers calculated the tidal impedance variation (TIV) for each image pixel in each recorded tidal breath and created 2D plots showing the distribution of tidal volume in the chest cross-section. They then quantified this spatial distribution using a series of established EIT measures: the centre of ventilation in the ventrodorsal (front-to-back) direction (CoVvd) and the right-to-left direction (CoVrl); and the dorsal and right fractions of ventilation.
The overall results from the male and female subgroups revealed significant differences in ventilation distribution between men and women. In the right-to-left direction, women exhibited a more symmetric distribution between the right and left lung regions than men, with CoVrl located more at the right side of the chest in male subjects than in female subjects. The right fraction of ventilation was also higher in men than in women.
Differences were less pronounced in the front-to-back direction, but still significant, with CoVvd predominantly located in the dorsal image half in both sexes, but more dorsally in men.
The researchers also calculated ventilation defect scores, a parameter that further defines the heterogeneity in ventilation distribution throughout the lungs. To calculate this score, they determined the fraction of ventilation in each image quadrant, and assigned a value of 0 (for a fraction of 0.15 or higher), 1 (between 0.10 and 0.15) or 2 (lower than 0.10) to each. Summing the four quadrant values gave the overall ventilation defect score.
They observed that ventilation distribution among quadrants was less heterogeneous in women than in men, with 83.4% of women exhibiting low ventilation defect scores (0 or 1), compared with 57.5% of men. A score higher than 1 was found in 42.5% of men but only in 16.6% of women.
Differences matter
The researchers conclude that ventilation distribution detected by EIT is affected by biological sex in this large group of quietly breathing male and female subjects, with the most striking variation the significantly higher right-to-left asymmetry seen in men than in women. They attribute this finding in part to differences in chest anatomy – the left ventricle is much larger in men than in women, even after normalization to body height.
Novel X-ray technology depicts real-time airflow through the lungs
Another possible cause may be breathing mechanics: differences in skeletal chest anatomy mean that women mainly perform thoracic breathing whereas men mainly exhibit abdominal breathing, which creates larger diaphragm motion. As EIT is sensitive to out-of-plane impedance changes, measurements may be affected by the movement of abdominal organs lying above and below the examination plane, particularly as this study used electrodes located at the lower part of the chest. But as the researchers did not monitor the type of breathing during the study, they cannot determine the exact role of this factor.
The findings reiterate the importance of accounting for biological gender when interpreting clinical chest EIT studies. The researchers point out the need for further clinical studies in lung-healthy subjects. “We need to perform large population studies to determine the reference values of several EIT measures for both sexes and also to clarify if sex differences exist when EIT examinations are performed in different body positions and chest sections,” Frerichs tells Physics World.



