ThinkQA Secondary Dose Check software provides quality assurance for every fraction of adaptive radiotherapy without impacting the clinical workflow

Adaptive radiotherapy, an advanced cancer treatment in which each fraction is tailored to the patient’s daily anatomy, offers the potential to maximize target conformality and minimize dose to surrounding healthy tissue. Based on daily scans – such as MR images recorded by an MR-Linac, for example – treatment plans are adjusted each day to account for anatomical changes in the tumour and surrounding healthy tissue.
Creating a new plan for every treatment fraction, however, increase the potential for errors, making fast and effective quality assurance (QA) procedures more important than ever. To meet this need, the physics team at Hospital Almater in Mexicali, Mexico, is using Elekta ONE | QA, powered by ThinkQA Secondary Dose Check* (ThinkQA SDC) software to ensure that each adaptive plan is safe and accurate before it is delivered to the patient.
Radiotherapy requires a series of QA checks prior to treatment delivery, starting with patient-specific QA, where the dose calculated by the treatment planning system is delivered to a phantom. This procedure ensures that the delivered dose distribution matches the prescribed plan. Alongside, secondary dose checks can be performed, in which an independent algorithm verifies that the calculated dose distribution corresponds with that delivered to the actual patient anatomy.
“The secondary dose check is an independent dose calculation that uses a different algorithm to the one in the treatment planning system,” explains Alexis Cabrera Santiago, a medical physicist at Hospital Almater. “ThinkQA SDC software calculates the dose based on the patient anatomy, which is actually more realistic than using a rigid phantom, so we can compare both results and catch any differences before treatment.”
For adaptive radiotherapy in particular, this second check is invaluable. Performing phantom-based QA following each daily imaging session is often impractical. Instead, in many cases, it’s possible to use ThinkQA SDC instead.
“Secondary dose calculation is necessary in adaptive treatments, for example using the MR-Linac, because you are changing the treatment plan for each session,” says José Alejandro Rojas‑López, who commissioned and validated ThinkQA SDC at Hospital Almater. “You are not able to shift the patient to realise patient-specific QA, so this secondary dose check is needed to analyse each treatment session.”
ThinkQA SDC’s ability to achieve patient-specific QA without shifting the patient is extremely valuable, allowing time savings while upholding the highest level of QA safety. “The AAPM TG 219 report recognises secondary dose verification as a validated alternative to patient-specific QA, especially when there is no time for traditional phantom checks in adaptive fractions,” adds Cabrera Santiago.
The optimal choice
At Hospital Almater, all external-beam radiation treatments are performed using an Elekta Unity MR-Linac (with brachytherapy employed for gynaecological cancers). This enables the hospital to offer adaptive radiotherapy for all cases, including head-and-neck, breast, prostate, rectal and lung cancers.
To ensure efficient workflow and high-quality treatments, the team turned to the ThinkQA SDC software. ThinkQA SDC received FDA 510(k) clearance in early 2024 for use with both the Unity MR-Linac and conventional Elekta linacs.
Rojas‑López (who now works at Hospital Angeles Puebla) says that the team chose ThinkQA SDC because of its user-friendly interface, ease of integration into the clinical workflow and common integrated QA platform for both CT and MR-Linac systems. The software also offers the ability to perform 3D evaluation of the entire planning treatment volume (PTV) and the organs-at-risk, making the gamma evaluation more robust.

Commissioning of ThinkQA SDC was fast and straightforward, Rojas‑López notes, requiring minimal data input into the software. For absolute dose calibration, the only data needed are the cryostat dose attenuation response, the output dose geometry and the CT calibration.
“This makes a difference compared with other commercial solutions where you have to introduce more information, such as MLC [multileaf collimator] leakage and MLC dosimetric leaf gap, for example,” he explains. “If you have to introduce more data for commissioning, this delays the clinical introduction of the software.”
Cabrera Santiago is now using ThinkQA SDC to provide secondary dose calculations for all radiotherapy treatments at Hospital Almater. The team has established a protocol with a 3%/2 mm gamma criterion, a tolerance limit of 95% and an action limit of 90%. He emphasizes that the software has proved robust and flexible, and provides confidence in the delivered treatment.
“ThinkQA SDC lets us work with more confidence, reduces risk and saves time without losing control over the patient’s safety,” he says. “It checks that the plan is correct, catches issues before treatment and helps us find any problems like set-up errors, contouring mistakes and planning issues.”
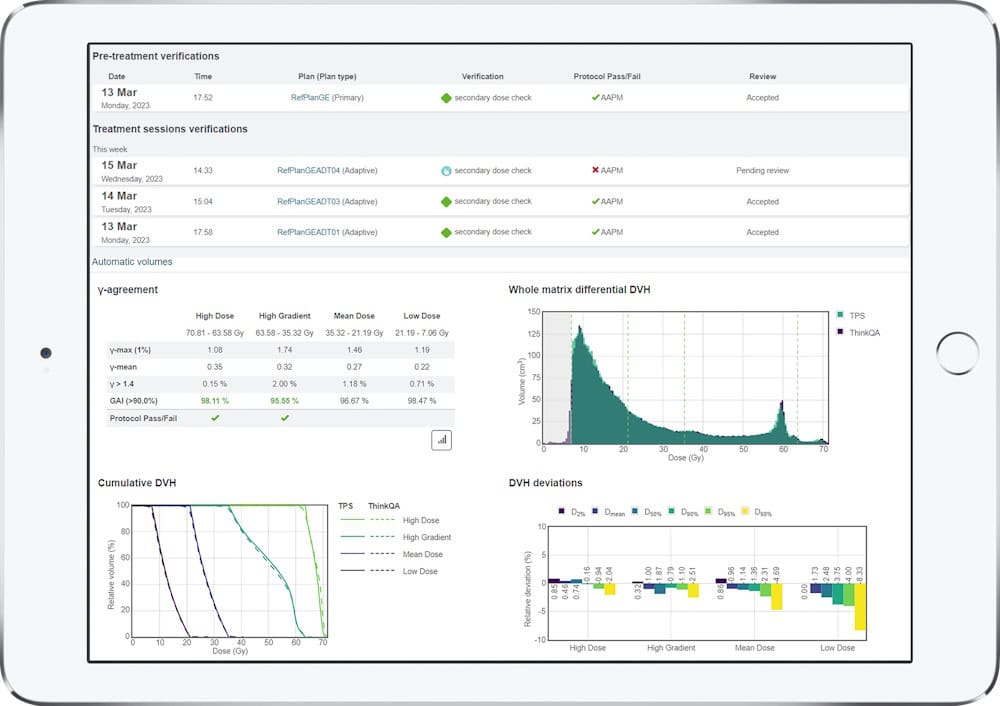
The software integrates smoothly into the Elekta ONE adaptive workflow, providing reliable results without slowing down the clinical workflow. “In our institution, we set up ThinkQA SDC so that it automatically receives the new plan, runs the check, compares it with the original plan and creates a report – all in around two minutes,” says Cabrera Santiago. “This saves us a lot of time and removes the need to do everything manually.”
A case in point
As an example of ThinkQA SDC’s power to ease the treatment workflow, Rojas‑López describes a paediatric brain tumour case at Hospital Almater. The young patient needed sedation during their treatment, requiring the physics team to optimize the treatment time for the entire adaptive radiotherapy workflow. “ThinkQA SDC served to analyse, in a fast mode, the treatment plan QA for each session. The measurements were reliable, enabling us to deliver all of the treatment sessions without any delay,” he explains.
Indeed, the ability to use secondary dose checks for each treatment fraction provides time advantages for the entire clinical workflow over phantom-based pre-treatment QA. “Time in the bunker is very expensive,” Rojas‑López points out. “If you reduce the time required for QA, you can use the bunker for patient treatments instead and treat more patients during the clinical time. Secondary dose check can optimize the workflow in the entire department.”
Importantly, in a recent study comparing patient-specific QA measurements using Sun Nuclear’s ArcCheck with ThinkQA SDC calculations, Rojas‑López and colleagues confirmed that the two techniques provided comparable results, with very similar gamma passing rates. As such, they are working to reduce phantom measurements and, in most cases, replace them with a secondary dose check using ThinkQA SDC.
The team at Hospital Almater concur that ThinkQA SDC provides a reliable tool to evaluate radiation treatments, including the first fraction and all of the adaptive sessions, says Rojas‑López. “You can use it for all anatomical sites, with reliable and confident results,” he notes. “And you can reduce the need for measurements using another patient-specific QA tool.”
“I think that any centre doing adaptive radiotherapy should seriously consider using a tool like ThinkQA SDC,” adds Cabrera Santiago.
*ThinkQA is manufactured by DOSIsoft S.A. and distributed by Elekta.