
Stereotactic ablative radiotherapy (SABR), in which high radiation doses are delivered over just a few fractions, requires management of intrafraction tumour motion to ensure accurate and safe treatment. Such motion management is generally provided by dedicated commercial real-time tracking systems. But according to new research from Australia, both multileaf collimator (MLC) tracking and gating can provide real-time motion adaptation on a standard linear accelerator. These low-cost strategies have the capability to make SABR treatments more accessible.
Writing in Radiotherapy and Oncology, researchers from the ACRF Image X Institute of the University of Sydney and four other Australian cancer treatment centres evaluated radiation doses delivered to 44 prostate cancer patients when using MLC tracking and gating with a standard linac. The patients were enrolled in the TROG 15.01 SPARK trial, which examined the use of kilovoltage (kV) intrafraction monitoring (KIM) to measure tumour position during treatment.
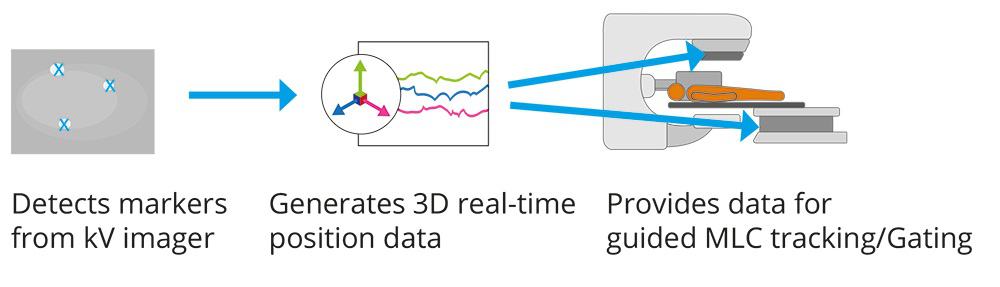
During the study, led by Paul Keall, professor of medical physics at the University of Sydney Medical School and director of the ACRF Image X Institute, and Jarad Martin, a radiation oncologist at Calvary Mater Newcastle, the researchers delivered 49 fractions using MLC tracking and 166 fractions using beam gating and couch shifts. They performed motion tracking with KIM, which uses the linac’s on-board kV imager to acquire patient images during treatment. Intrafraction KIM-guided motion adaption was then performed using MLC tracking for 10 patients or gating for 34 patients. Of the 166 gated fractions, 65 included prostate motion that exceeded established thresholds and required treatment interruptions.
The researchers estimated the radiation doses that would have been delivered without motion adaptation and compared these with doses delivered when employing MLC tracking or gating. To evaluate the efficiency of gated treatments, they also calculated the time required to gate and perform a couch shift for each fraction.
Gated treatments proved to be efficient, taking between 5 and 19 min to complete, compared with 2 to 17 min for MLC tracking. Couch shift interruptions lasted between 1 and 4 min. Because KIM calculated the new couch position, the treatment team only needed enter the new values into the treatment system.

Both MLC tracking and gating delivered similar radiation doses, and both delivered doses closer to the treatment plans than if no motion adaptation strategy had been used. “Both methods were effective at improving dose delivery accuracy that is crucial for high-dose treatments,” says first author Emily Hewson. “While MLC tracking had a slight dosimetric improvement compared with gating, this difference was small, so either method could be used to provide accessible SBRT treatments for prostate cancer.”
Hewson notes that the variance of dose differences from the treatment plan was larger with gating than MLC tracking for the bladder and rectum. “Data suggest that while both strategies would perform similarly on average, gating would result in doses that deviated more from the plan for the worst cases,” she adds.
The researchers suggest that MLC tracking might have been more accurate if a leaf width smaller than 5 mm had been used. “Smaller MLC leaves offer higher beam adaptation accuracy, which would benefit the small, slow motion that the prostate undergoes,” explains Hewson. “Another alternative to improve accuracy would be to integrate MLC tracking with a real-time couch tracking method in the future to compensate for the finite MLC leaf width.”
Addressing the complexity of each strategy, Hewson says that treatment planning and implementation were comparable, but that the underlying software and quality assurance processes for MLC tracking are more complex than gating.
“MLC tracking requires complex software to automatically adapt the treatment beam in real time, requiring more commissioning. Also, each patient plan requires pre-treatment dosimetric quality assurance,” she explains. “But implementing MLC tracking during treatment simply requires the treatment team to open the MLC tracking software; adaptation is automated. Gating requires more intervention by the treatment team if tumour motion exceeds the designated threshold.”
The researchers say that the accuracy of each adaptation method will be limited by the accuracy of the tumour localization method. The 3D tumour localization accuracy of KIM in the trial was quantified to be 0.0±0.5 mm, 0.0±0.4 mm, and 0.0±0.5 mm in the anteroposterior, left–right, and superior-inferior directions, respectively.
Real-time image-guided ART achieved on a standard linac

“KIM provides real-time tumour position in six degrees-of-freedom using fiducial markers that are MR-compatible and smaller than beacons used with some commercial systems,” the team write. “And because KIM utilizes the on-board kV imager that is already equipped on modern linacs, it potentially will allow widespread implementation of SABR.”
“Our implementation of KIM to monitor tumour motion, combined with either gating or MLC tracking improves the availability of intrafraction motion adaption for all clinics with standard treatment machines,” says Hewson. “One of the major barriers to implementing real-time adaptive radiotherapy in many countries has been a lack of finances and resources. The adaptive methods we compared could potentially overcome these obstacles and bring intrafraction motion adaptation into standard clinical practice at any cancer treatment facility that treat patients using a modern linear accelerator.”



