Using advanced imaging to predict the likelihood of a malignant brain tumour recurring after radiation treatment could enable creation of a more effective treatment plan. With this aim, researchers at the University of Copenhagen have developed a model that uses pre-treatment PET and MRI to create patient-specific maps of recurrence probability for glioblastoma tumours (Eur. J. Nucl. Med. Mol. Imaging 10.1007/s00259-018-4180-3).
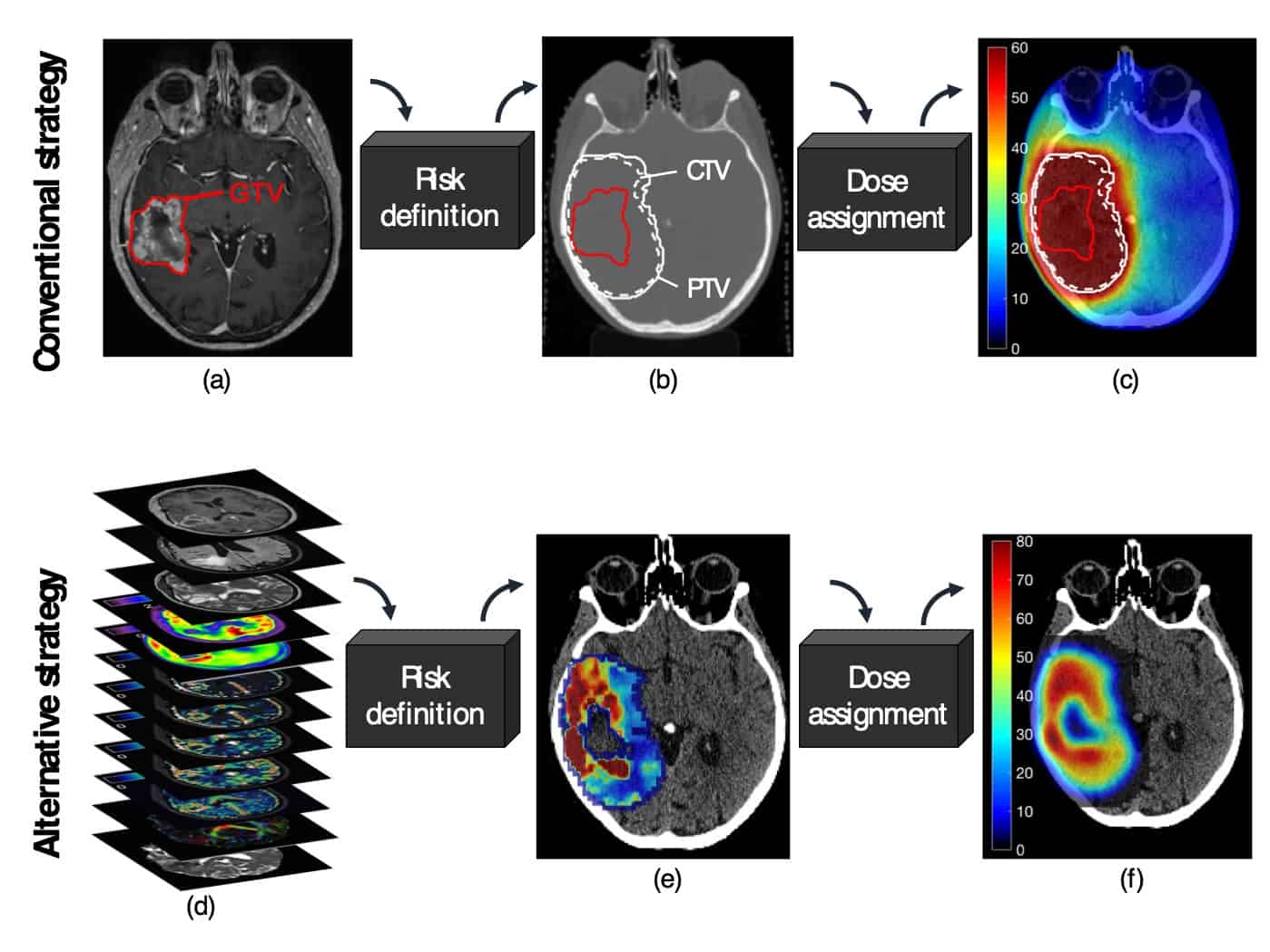
Radiotherapy for the brain cancer glioblastoma is conventionally planned using anatomic MRI to define radiation dose targets. Failure rates are high, however, often attributed to the target not receiving a high enough radiation dose — a trade-off of minimizing toxicity to surrounding healthy brain tissues. If a more specific target volume could be determined, identifying the area exhibiting a high risk of recurrence, this could enable delivery of a more precise, and potentially more effective, patient-specific radiation dose.
Principal investigator Michael Lundemann, a clinical scientist in biomedical engineering at Rigshospitalet, and colleagues compared multi-parametric PET and MR scans, performed prior to and after radiotherapy, to determine whether the risk model could predict a voxel-wise probability of tumour recurrence
The researchers included nine patients in the analysis. All patients had undergone a routine MRI for radiotherapy planning, a sequential 18F-FET-PET/CT scan, where the CT was used for radiation dose calculation and PET attenuation correction, and a simultaneous 18F-FDG-PET/MRI scan. These images yielded 63,862 voxels within the clinical target volume (CTV), of which 6944 voxels registered recurrent tumour. Five patients also developed recurrent lesions outside the CTV, but these were not included in the analysis.
The patients had surgical resection, followed by 60 Gy of radiotherapy and up to six cycles of chemotherapy. Tumour progression occurred between 124 and 545 days (median time of 357 days) and the overall survival was 631 (range: 290–766) days.
For the image analysis, the researchers separated the voxels within the CTV into four regions-of-interest (ROIs): contrast-enhanced lesion, non-enhancing lesion, normal appearing white matter and normal appearing grey matter. They delineated recurrent tumour volume locations, and assessed voxel-wise correlations between imaging parameters for each of the four ROIs, categorizing them as recurring or non-recurring. They created maps of tumour recurrence probability from the pre-treatment multi-parametric images, and developed four voxel-wise binomial logistic regression models (one for each tissue class).
The research showed that:
- Voxels included in the recurrent tumour volume at the time of recurrence showed larger 18F-FET-uptake than voxels in non-recurring parts of the CTV;
- An increased uptake of both 18F-FDG and 18F-FET was observed in recurring voxels that originated from either the contrast-enhanced lesion or the non-enhancing lesion;
- An increased vascular permeability was observed in recurring voxels that originated from otherwise healthy appearing grey and white matter;
- Significant median differences between recurring and non-recurring voxels were also observed for fractional anisotropy, mean diffusivity, mean transit time, extra-vascular and extra-cellular blood volume derived from scans prior to chemo-radiotherapy.
Overall, 18F-FET proved to be the most important parameter for recurrence prediction. When all models of recurrence probability were combined, the area under the ROC curve (AUC) for prediction of recurrence was 0.77.
“Our study could be a first step to enable a higher degree of patient-specific planning of dose delivery by specifically targeting areas with high risk of recurrence,” wrote the authors. “Our results are based on a low number of patients and need further validation before the clinical utility can be tested in a prospective setting. However, the results are encouraging and serve as a starting point for further studies.”
The authors do recommend use of a simpler, shorter and more manageable multi-parametric imaging protocol prior to radiotherapy. This would include PET/MRI employing 18F-FET PET, dynamic contrast-enhanced MRI and possibly diffusion weighted imaging.
“If we know in advance in which parts of the brain a tumour is more likely to recur, a radiation oncologist could decide to increase the dose delivered to high-risk areas and lower the dose to low-risk areas,” Lundemann tells Physics World. “We hypothesize this could lead to a better local tumour control without damaging healthy parts of the brain and in turn extend patient survival.”
Lundemann says that he is continuing research within brain tumours, while colleagues in his department are investigating tumour recurrence in head-and-neck tumours, lymphomas and cervical tumours.



