Mammography screening has been shown to reduce mortality from breast cancer. But mammograms are far from perfect, with one study finding that only 46% of detected cancers were true positives, while 22% of genuine cancer cases were missed. The problem arises because the soft tissue in the breast provides limited X-ray contrast and the two-dimensional projection used in mammography fails to clearly depict the complex structure of the breast.
Dedicated breast computed tomography (CT) provides volumetric data, thereby eliminating challenges arising from tissue overlap and breast compression. But it does not solve the fundamental contrast limit of attenuation-based X-ray imaging. To overcome this limit, researchers have turned to phase-contrast X-ray imaging, a technique that exploits refraction and interference effects to create images with significantly higher contrast and resolution. Such improvements could help detect tumours at an earlier stage and improve the chances of survival.
To date, phase-contrast X-ray imaging has been constrained by the need for highly coherent X-ray sources such as synchrotrons. Another approach is grating interferometry-based phase-contrast CT (GI-CT), which works with conventional X-ray tubes but requires high X-ray doses. Now, a research team headed up at the Paul Scherrer Institute (PSI) and ETH Zurich has developed a GI-CT technique that’s more dose efficient than conventional CT for breast imaging under near-clinical conditions,
Grating interferometry (which was first demonstrated at PSI) works by placing a series of diffraction gratings, with a line spacing of a few microns, between the X-ray source and the detector. The gratings introduce an interference pattern into the X-ray beam, which is then distorted when the beam passes through the sample. Refraction on large-scale structures causes the pattern to shift laterally (the phase contrast), while refraction on small unresolvable structures blurs the pattern (the dark-field signal). Analysis of the distorted pattern therefore yields three potential images: based on attenuation, phase contrast and the dark-field signal.
Performance assessment
Marco Stampanoni, professor of X-ray imaging at ETH Zurich and head of the research group at PSI, and colleagues constructed a GI-CT system based on a tungsten-anode X-ray source (operated at a typical breast CT energy of 70 kVp), a photon-counting detector with an active area of 195 × 19.2 mm, and a Talbot–Lau interferometer based on commercially available gratings with a 4.2 µm pitch.
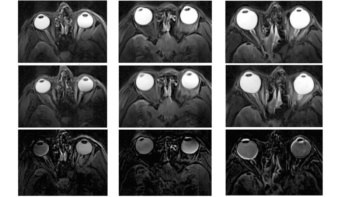
The researchers used the device, described in Optica, to image a human breast sample, with an average delivered dose ranging from 5.5 to 219 mGy. They reconstructed images using both attenuation and phase contrast and found that the visual quality of both contrasts increased with delivered dose. At the lowest dose, the phase-contrast image appeared inferior to the attenuation-contrast image; however, for the higher dose, the PC image appeared superior.
To effectively resolve the morphology of the breast, a contrast-to-noise ratio (CNR) of five between adipose and glandular tissue is needed. To decrease the CNR to that value, the researchers filtered the reconstructed volumes with a Gaussian kernel. For each image, they determined the size of the kernel (a lower limit on the resolution) needed to achieve this CNR and the necessary dose at this resolution.
They found that the dose requirement increased more rapidly for attenuation-based than phase-based images. At a resolution of 214 µm or above, phase-contrast images were sharper than images derived solely from attenuation at the same dose.
The researchers also compared GI-CT to conventional attenuation-based CT. Even though GI-CT only utilizes half of the photon flux, fusing the attenuation- and phase-contrast signals provided sufficient information to compensate for this loss. “We demonstrated that we get more information from refraction than we lose due to half of the photons being absorbed by the analyser grating,” explains lead author Michał Rawlik.
For spatial resolution better than 263 µm and absorbed dose of 16 mGy (both within clinical ranges), GI-CT outperformed conventional CT. For sharper kernels, GI-CT exhibited increasing benefit, for example, requiring only 53% of the dose at 150 µm. The team’s goal is to reduce the dose by a factor of two to three compared with conventional X-rays, while maintaining the same resolution. As the sensitivity of GI-CT is constrained by the grating fabrication, improvements in fabrication technology should take GI-CT closer to that limit and, with smaller grating pitches, possibly beyond it.
Phase-contrast imaging could improve breast cancer diagnosis

As this study examined a breast tissue sample with no tumour or microcalcifications, the researchers did not incorporate the dark-field signal in their analyses. Future studies on pathological samples will allow them to investigate the benefit of the dark-field signal for breast CT. They also plan to examine the impact of breast density and how the increased CNR correlates with diagnostic accuracy.
The researchers note that GI-CT is compatible with conventional CT scanners, making it suitable for widespread use in hospitals and immediately applicable to dedicated breast CT systems. They have now developed two clinical GI-based investigational devices, including a 2D mammography system retrofitted with a grating interferometer that’s installed in University Hospital Zürich. This device has received Swissmedic approval, and a clinical study is planned to start this year. The other is a phase-contrast breast CT device, which the team is currently commissioning in the lab at ETH Zurich, with device approval planned by the end of 2024.