Fever, an elevated body temperature of about 38.0–38.3 °C or above, is one of the most common symptoms in children presenting at the hospital. Fever can arise due to a variety of conditions – most commonly infection, followed by autoimmune disease and then malignancy. But in around half of infants up to three years old, and 10–20% of all children, no definitive cause is found, despite extensive diagnostic and laboratory tests. This condition referred to as fever of unknown origin (FUO).
In adults with FUO, PET/CT with the tracer 18F-FDG has been used to diagnose focuses of infection or inflammation. In children with FUO, however, studies are scarce and its usefulness remains unestablished. Now a team from University Medical Center Groningen (UMCG) has examined a large group of children with FUO to determine the value of FDG-PET/CT in finding the cause of fever (Eur. J. Nucl. Med. Mol. Imaging 10.1007/s00259-020-04707-z).
“Fever can be caused by many different diseases, some of which could be fatal if left untreated,” explains first author Jordy Pijl. “If the cause of fever is unknown, it can be very difficult to start the right treatment, leading to increased morbidity or even mortality of patients.”
Data mining
Pijl and colleagues searched UMCG’s electronic patient database for patients aged up to 18 years who had undergone FDG-PET/CT for fever evaluation between 2010 and 2019. For the study, they examined the scans of 101 patients with FUO (fever for eight or more days) and nine patients with fever without source (FWS, fever without a clear source for less than eight days).
In 68 of the 110 patients (62%), a definite cause of fever was found, with FDG-PET/CT identifying the cause in 53 of these cases. Common diagnoses included endocarditis, systemic juvenile idiopathic arthritis and inflammatory bowel disorder. In 42 patients (38%), no cause of fever was found on FDG-PET/CT or any other diagnostics and the children remained as FUO.
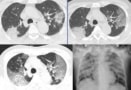
In one example case (shown in the above image), a 9-year-old boy presented at the hospital with anorexia, weight loss, fatigue and intermittent fever up to 39.5 °C. He had experienced these symptoms episodically over the past 18 months, but had no definite diagnosis. FDG-PET/CT showed extensive FDG uptake throughout the entire colon, suggesting inflammatory bowel disorder; intestinal biopsy established the final diagnosis of Crohn’s disease.
Based on the reference standard (the final diagnosis at the patient’s discharge), 53 FDG-PET/CT results were true positive, 10 were false positive, 38 were true negative and nine were false negative. These findings correspond to a sensitivity of 85.5%, specificity of 79.2%, positive predictive value of 84.1% and negative predictive value of 80.9%.
The researchers point out that, as the false negatives illustrate, it’s important to remember that not all cases of FUO can be diagnosed with FDG-PET/CT. They suggest precautions that could help avoid unnecessary false negatives, including patients sticking to low-carbohydrate diets, especially when a focus of fever is suspected in tissues with high metabolic activity, and minimizing corticosteroid dose, especially when vasculitis is suspected.
In 58 out of the patients (53%), FDG-PET/CT led to treatment modifications, including a change in antibiotics, starting immunosuppressive therapy and starting treatment with a non-steroidal anti-inflammatory drug.
Associated factors
The researchers also used multivariate logistic regression to look for clinical parameters associated with FDG-PET/CT performance. They found that the level of C-reactive protein was positively associated with FDG-PET/CT determining a true positive focus of fever, while leukocyte count was negatively associated with finding a true positive. No other factors were significantly associated with outcome, making it a challenge to identify FUO patients who may likely benefit from FDG-PET/CT investigations.
CT traces disease progression in novel coronavirus
While diagnostic tests such as a chest X-ray or urinalysis are quick, easy to perform and relatively cheap, and should thus be considered first, FDG-PET/CT provides a valuable diagnostic tool for evaluating children with FUO, the authors conclude. “FDG-PET/CT is a rapidly developing technique that can provide a quick full-body evaluation with less and less radiation, so in the future, it will likely climb up the diagnostic ladder of fever,” says Pijl.
“Now that we have looked into children with all causes of fever, we would like to focus on evaluating the use of FDG-PET/CT for specific causes of fever,” he tells Physics World. “Also, we are planning studies to evaluate the newest PET/CT scanners that can perform a scan in less time and with less radiation, thereby further establishing the role of FDG-PET/CT in diagnosing patients – and especially children – with fever or other symptoms of diseases.”