Obstructive sleep apnoea (OSA) is a sleep disorder in which the throat muscles relax and block the airway during sleep, causing pauses in breathing. If left untreated, OSA can lead to serious health problems. A research team led by Mingjiang Wang at the Harbin Institute of Technology, Shenzhen in China, in collaboration with Huizhou University, has now come up with a new method for detecting OSA – based on recordings of the subject snoring.
“OSA is a common yet underdiagnosed sleep disorder,” explains first author Heng Li. “The clinical standard for diagnosis is polysomnography [PSG], which is expensive, time-consuming and unsuitable for large-scale or home-based screening.”
PSG collects multiple physiological signals via various sensors that patients wear while asleep, potentially disrupting their sleep patterns. “Therefore, we aim to develop a non-contact detection method using snoring, which is a typical symptom of OSA and can be recorded contactlessly using a microphone,” says Li.
The acoustic patterns of snoring, produced by the vibrations of upper airway, contain markers that reflect airway narrowing and collapse. However, developing a reliable snoring-based detection model is challenging, as labelled snoring datasets are scarce and snoring sounds vary greatly between individuals.
In this study, published in Physiological Measurement, the research team uses a pretrained audio model called Wav2vec 2.0 to address these challenges. By transferring acoustic knowledge learned from large-scale unlabelled speech and audio data, the model removes the need for labelled snoring datasets.
Wav2vec 2.0 was originally designed for speech recognition and is computationally intensive, making it unsuitable for routine OSA monitoring. Thus the team adapted it for snoring sounds, removing layers more relevant to speech recognition while retaining acoustic features relevant to snoring pathology, aiming to lower the computational cost.
“We do not use the pretrained model directly,” Li explains. “Instead, we prune higher speech-related Transformer layers and fuse low- and mid-level representations, so that the model emphasizes snoring-related acoustic information.”
Constructing a snoring dataset
In collaboration with the Shenzhen People’s Hospital, the team collected sleep recordings from 100 individuals with apnoea-hypopnea indices (AHI) ranging from 2.4 to 68.3 events/hour. AHI – defined as the average number of apnoea (where breathing stops completely) and hypopnoea (shallow breathing) events per hour of sleep – is used to classify OSA from normal (AHI of below 5) through to severe (30 or above).
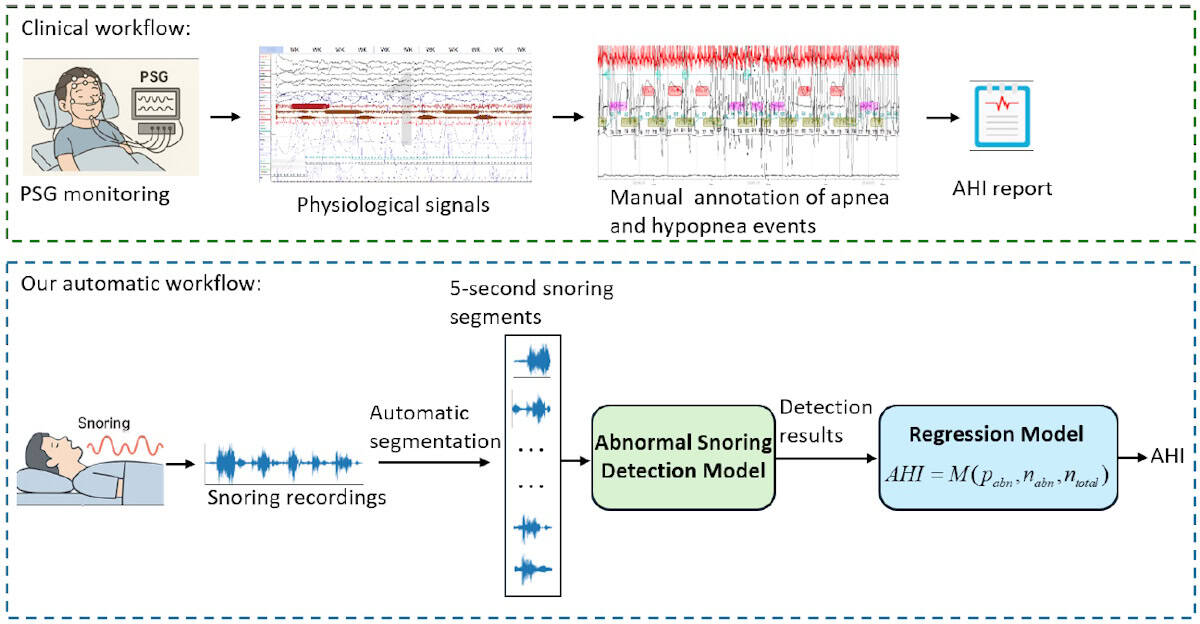
All subjects slept in hospital wards and were also monitored with a PSG device during sleeping. Sleep physicians then used the PSG data to annotate the audio recordings with apnoea and hypopnea events. Each recording was divided into 5-s audio segments and assigned as either abnormal, if they included apnoea/hypopnoea events, or normal.
To evaluate their framework’s ability to detect abnormal snoring, the researchers compared it against five other pretrained audio models. They first ran a subject-dependent evaluation, in which random audio segments from all subjects were used for training, validation and testing. All models performed well – as expected when the training and test data come from the same subjects – but the adapted Wav2vec 2.0 model achieved the highest accuracy and sensitivity.
The team then performed a subject-independent evaluation, which better reflects a real-world scenario, with each subject’s data randomly assigned to the training, validation or test set. Here, the existing methods exhibited a reduced accuracy of between 65% and 71%, while the new model retained an accuracy of 73.95%.
“In subject-independent testing, this adapted model achieved better performance than the compared baseline models, suggesting improved generalization to unseen subjects,” says Li. The team’s model was also significantly more computationally efficient, an important factor for OSA screening in home-based or resource-limited scenarios.
AHI estimation
Finally, the researchers designed a snoring-based AHI estimation framework, using their detection model to identify abnormal snoring segments and calculating a ratio-based statistic – the number of abnormal segments divided by the total number of segments – to quantify OSA severity. They then used four common linear regression models to estimate AHI for individual subjects.
Low-cost wearable devices quantify breathing activity while you sleep

All models demonstrated reasonable accuracy and good correlation between predicted and PSG-derived AHI values. The mean absolute error was roughly 11 events/h, which means that the estimated AHI may deviate from the true value by 11 events per hour of sleep and could (if near a threshold between categories) result in an incorrect severity diagnosis. However, while the current model is not yet precise enough for clinical diagnosis, it could prove ideal as a potential tool for home-based OSA screening or pre-screening.
The researchers are now investigating how to more effectively apply pretrained audio models to clinical snoring analysis. “We are focused on making these models lighter and more suitable for home-based screening, while validating their effectiveness across large, multicentre datasets,” Yun Lu, one of the corresponding authors from Huizhou University, tells Physics World. “Additionally, we plan to improve the accuracy of AHI estimation by integrating snoring-based predictions with additional non-contact physiological information.”