A lively debate at the ESTRO 2026 meeting concluded with nearly 70% of the audience backing upright proton therapy as a mainstream treatment option by 2035

Two years ago, the ESTRO 2024 meeting in Glasgow dedicated a conference session to the discussion of upright radiotherapy. In particular, the speakers pondered whether this emerging technique – in which patients are treated sitting up rather than lying down – offers hope of increasing access to advanced radiotherapy, or whether it’s merely hype.
Things have moved on since then. Leo Cancer Care introduced its upright photon therapy system, Grace, and received commercial approval in the US and (just last week) Europe for its Marie upright positioning and CT system. Stanford Medicine recently unveiled the world’s first ultracompact proton therapy facility, pairing Mevion Medical Systems’ compact S250-FIT proton therapy system with the Marie platform. Meanwhile, the body of published research on the feasibility and patient experience of upright treatments continues to grow.
At this year’s ESTRO 2026 meeting in Stockholm, the theme was revisited by four experts in the field, who debated the motion that “Upright radiotherapy will be a mainstream and standard radiotherapy delivery option in 2035”.
The customary pre-debate vote revealed that just one quarter of the audience thought that photon-based upright radiotherapy would become mainstream, with the remainder believing that it would remain a niche technique. When it came to upright proton therapy, however, the vote was split roughly 50:50. So could the speakers persuade the attendees to change their minds?
Patient-centred care
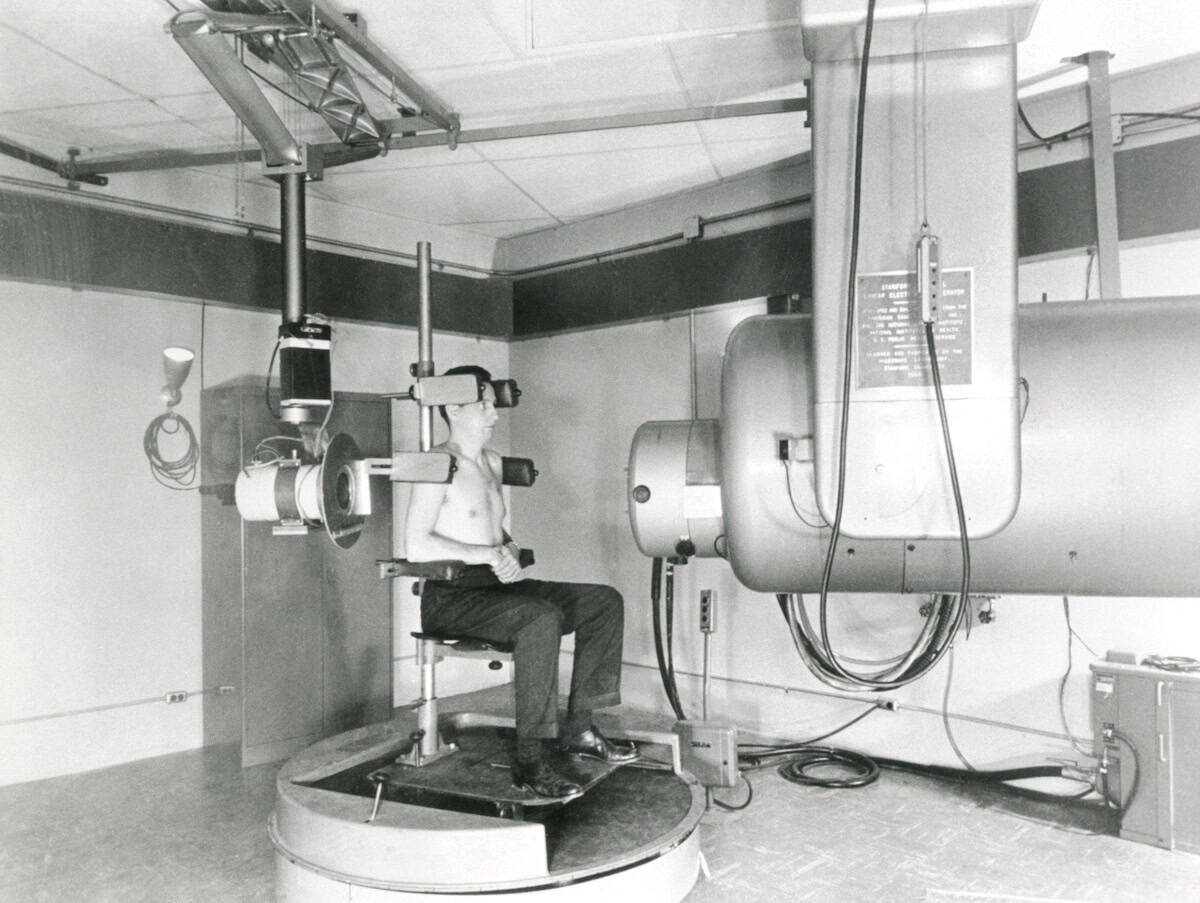
The debate began with Tomas Kron from the Peter MacCallum Cancer Centre in Australia arguing the case for upright X-ray radiotherapy. He pointed out that upright positioning is not a new idea. “Historically, photons and upright have been around for a very long time. It has been, if not standard practice, widely used. But what role will it play in 2035?”
Kron described a clinical imaging trial underway at Peter Mac investigating upright cone-beam CT for planning lung cancer radiotherapy. The study showed that image quality was good enough for adaptive treatment planning, and that the lung was expanded and moved less in the upright position. Kron noted that patient setup and imaging was “really, really easy”, taking just a few minutes.
But what’s more important, he emphasized, is the patient experience. Patients treated while sitting up can maintain eye contact with the doctors throughout, they feel more involved and empowered, with one patient commenting: “My breathing was strong, I felt comfortable, the band around my chest was giving me a bear hug.”
“It’s really all about patient-centred care. Physical comfort and emotional wellbeing are top priorities,” Kron said. “Clearly, in an upright scenario this is much more likely to be the case.”
Upright radiotherapy offers many other unique features, including anatomical advantages and the ability to customize the chair, for example, for bariatric or paediatric patients. An upright treatment system is also more compact than a couch-based machine, requiring a smaller bunker. It could also be used as a mobile radiotherapy unit, said Kron – reducing the need for patient travel.
Kron’s team found that 80–90% of their patients could be treated just as well with upright radiotherapy as supine (lying down). “There are anatomical advantages with upright, there are patient preferences, there are economic benefits. What’s not to like,” he concluded.
The myth of mainstream
“Upright radiotherapy will not be mainstream and standard,” declared the second speaker, Livia Marrazzo from the University of Florence in Italy.
“Mainstream means widely adopted, used across the majority of radiotherapy centres, the default in clinical practice … and standard is even stronger, backed by clinical evidence, guideline-endorsed, reproducible and validated,” Marrazzo told the delegates. “It’s not ‘it works in some centres, is technically feasible, has early adopters, may have advantages for some patients’. But that is where we are with upright radiotherapy.”

From a practical standpoint, most of the roughly 16,000 radiotherapy systems worldwide are linac-based recumbent machines with a typical lifecycle of 10 to15 years. Many were recently replaced with supine systems optimized for intensity-modulated and image-guided radiotherapy. “The installed base is locked into supine geometry for another full cycle,” Marrazzo explained.
She refuted many of the advantages proposed by Kron. “We have limited clinical evidence supporting comfort advantages,” she said. “It may benefit specific patient groups and conditions, but this doesn’t mean mainstream.” Overall, clinical experience is limited, with no comprehensive evaluations of plan quality and no comparative clinical studies.
She highlighted the particular challenges of breast cancer treatments, which account for 25-30% of cases in her radiotherapy department. “When we place a breast cancer patient upright, we lose the natural breast separation, so have much more difficulty in hitting the target and avoiding the contralateral breast,” she explained. “This exemplifies how upright is not a plug-and-play replacement for a conventional supine workflow.”
“Are we sure we would like to have upright as the standard radiotherapy delivery option by 2035 or do we want to push our efforts somewhere else?” Marrazzo concluded. She would prefer a focus on introducing technologies such as AI-driven planning and contouring, fully adaptive workflows, ultra-hypofractionation or biology-guided treatment adaptation. “These are all solutions that can be software-driven, scalable and compatible with existing supine infrastructure.”
The motion for protons
With half of the audience already agreeing that upright proton therapy will become mainstream, Petra Trnkova from Czech Technical University had perhaps a slightly easier task as she presented the case for upright protons. Nevertheless, she began by suggesting that her opponents are simply “scared of progress and won’t accept that, even without evidence, we can move forward in radiotherapy”.
Trnkova reiterated the benefits of upright radiotherapy cited by Kron: favourable patient anatomy, lower installation cost, improved sustainability, and patient-centric management. “For proton therapy, these improvements are much more significant,” she noted.
For starters, upright systems could help address the massive disparity in access to proton therapy around the globe. Sharing a map showing how proton therapy facilities are mostly distributed in wealthy countries, Trnkova noted: “My opponents may tell you that it’s not possible to do this by 2035, but when you look at this map, I ask you, can we wait any longer?”

Increasing access to proton facilities is enabled by the extreme size reduction when eliminating the need for a large rotating gantry, enabling proton therapy systems small enough to fit in a standard linac vault. Upright proton therapy can also reduce machine complexity, increase rotation speed and lower energy consumption – reducing costs, improving system upgradeability and increasing environmental sustainability.
“Another consequence of smaller facilities is we can really have patient-centred care,” Trnkova added. Recalling the 10 to 15 year linac lifetime mentioned by Marrazzo, she suggested another option: “You can replace your linac with proton therapy. Then you can have the full set of treatments available for each patient”.
Upright proton therapy could also ease the introduction of new treatment techniques, such as proton arc therapy, which offers dosimetric benefits over intensity-modulated proton therapy, but it is difficult to deliver with a gantry. It could also enable in vivo dosimetry, using shoot-through protons for range verification, or mixed-beam delivery of protons and photons.
“Upright positioning offers many opportunities, it’s the only way towards the democratization of proton therapy,” Trnkova concluded. “Stop asking what opportunities upright radiotherapy brings, start asking what you can do to bring it faster to clinical practice.”
The reality check
The final speaker, Carles Gomà from Clinic Barcelona in Spain, reflected upon what makes a good radiotherapy system. “In my view, it’s a three-legged stool: beam delivery, imaging and immobilization,” he said. “And progress comes with a combination of the three.”
For example, focusing too heavily on beam delivery and imaging can lead to immobilization being forgotten. “Immobilization means comfort, and if we are comfortable, we are still,” Gomà explained. “I cannot care less how many papers say patients are more comfortable in an upright position,” he added, pointing out that people will pay five times more to fly in business class where they can lie down.
The other reason cited for moving to upright proton therapy is its lower cost. “But is proton therapy expensive?” Gomà asked. He described the situation in Catalonia, which has a population of eight million and in 2018 spent Euro 42.2M on external-beam radiotherapy. “This is exactly the same cost as one immunotherapy drug for the same population,” he pointed out. “Proton therapy is not expensive; photon therapy is ridiculously cheap.”
Gomà also considered whether “suboptimal protons” are better than photons. “I’m going to answer no,” he said, describing two recent phase III, randomized trials comparing photons with protons for oropharyngeal cancer. The US trial concluded that proton therapy provides a new standard-of-care option, but the UK trial reported no difference between the two modalities.
“Let’s learn from history and not repeat the same mistakes,” he concluded. “True progress is improvement without compromise. If we want to make the stool higher, we have to work on all three legs at the same time.”
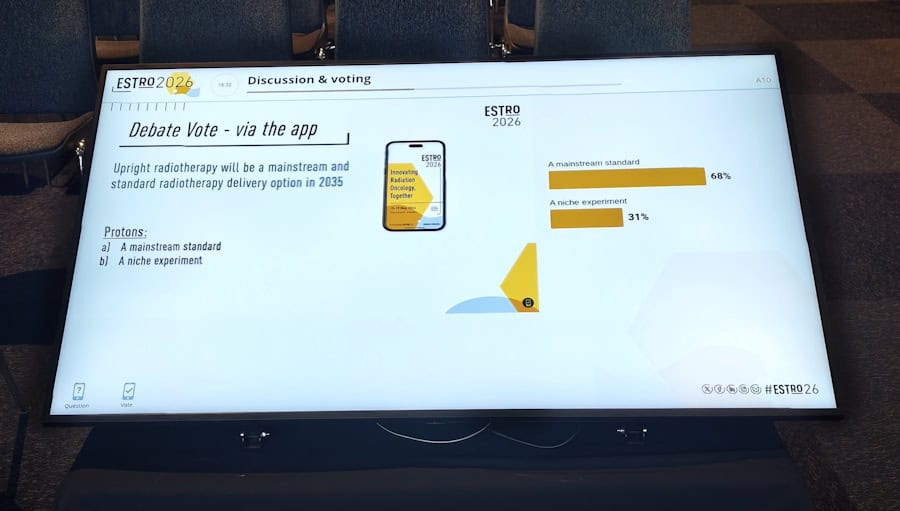
The debate concluded with decisive a final vote: while support for upright photon therapy reduced a little, over two-thirds of the audience believed that upright proton therapy will indeed become mainstream and standard by 2035.
Writing on LinkedIn, session co-chair Ye Zhang from the Paul Scherrer Institut noted: “The debate sparked an inspiring shift in perspective, with final voting showing slightly increased scepticism toward mainstream upright photon therapy (dropping from 23% to 18% support), but a dramatic surge in favour of upright proton therapy, which jumped from 47% to a 69% majority.”



