Cancer is a major healthcare concern worldwide, with 20 million new cases per year expected by 2025. Recent reports suggest that around 70% of the 7 million yearly cancer deaths occur in low- and middle-income countries (LMICs), and that 60% of cancer patients in such countries will require radiotherapy.
Intensity-modulated radiotherapy (IMRT) can increase a patient’s quality-of-life by sparing more normal tissue, while also reducing costs associated with managing toxicities. But while IMRT is available in essentially all radiotherapy clinics in high-income countries, it is largely absent in vast regions of LMICs. One obstacle is that most IMRT systems use multileaf collimators (MLCs), which contain hundreds of moving parts that need to be maintained to strict tolerances.
A team headed up at the University of Washington Medical Center has come up with a simple and cost-effective alternative: replace the moving MLCs with a ring of physical compensators. Importantly, the proposed device can be retrofitted to existing linac and cobalt teletherapy units – allowing clinics to add IMRT without having to purchase a new treatment system (Med. Phys. 10.1002/mp.12985).
“The overall goal of this project is to improve access to radiotherapy in low- and middle-income countries,” said senior author Eric Ford. “Due partly to the successes in dealing with infectious diseases in these parts of the world, cancer is becoming a big problem and many people have no access to care. To me, that is a problem worth solving.”
Reusable beads
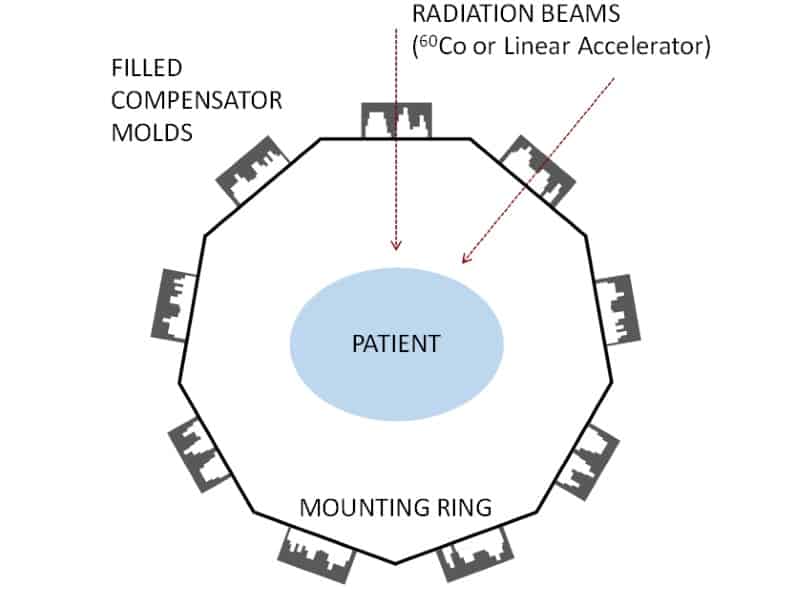
The compensators comprise plastic moulds, which are lightweight and easy to manufacture, filled with attenuating material such as tungsten beads. After each treatment the attenuator can be emptied from the moulds and re-used for another patient, minimizing the required amount of expensive attenuating material.
The compensators are mounted around the patient on a ring structure. The treatment gantry rotates around the ring and delivers each beam through each compensator in turn. Compared with MLCs, compensators offer simplicity, lower cost, streamlined QA and more efficient use of MUs. Another advantage is that the compensators do not need to be manually exchanged between delivery of each field, greatly increasing treatment efficiency.
To assess the dosimetry of this new set-up, the researchers used the Pinnacle treatment planning system to create plans for 60Co teletherapy beams used with the compensator. They chose a 60Co system as these are widely used in LMICs, and present the most challenging scenario due to their unfavourable depth-dose characteristics and large source sizes.
The researchers generated 60Co-compensator IMRT plans for five head-and-neck cancer and five gynaecological cancer patients, and compared these to MLC-based plans using a 6 MV linac. Ford noted that the treatment planning process is similar to that for standard IMRT.
“Inverse planning is performed and an idealized fluence map made,” he explained. “At this point the fluence map would normally be turned into a pattern of beam shapes using MLCs. Instead, we turn it into a compensator shape. Some treatment planning systems have this capability already, but even in those that do, it is not well developed. More work needs to be done to refine it.”
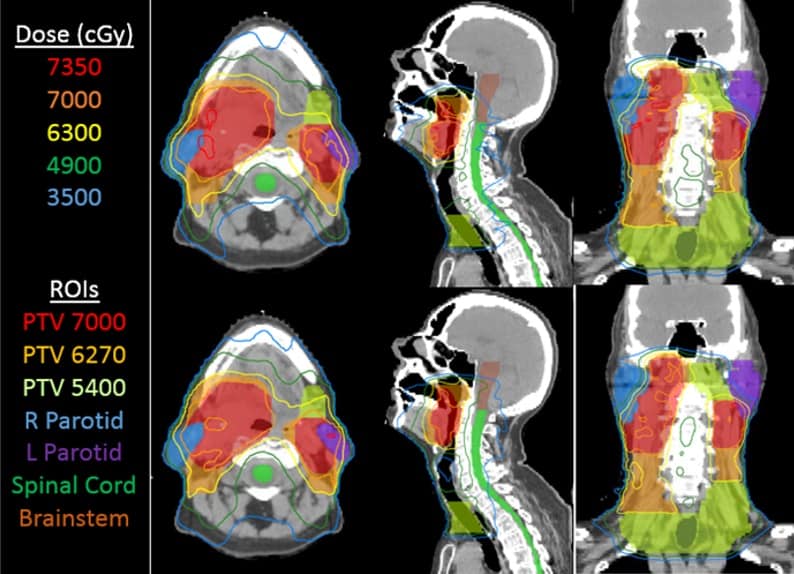
Comparing dose distributions revealed that 60Co-compensator plans had, on average, equivalent planning target volume (PTV) coverage to the MLC plans. The 60Co-compensator plans had higher mean parotid dose (for head-and-neck cases) and higher rectum D60% (for gynaecological cancers), but the differences in organ-at-risk (OAR) dosimetric endpoints were clinically acceptable. The 60Co-compensator plans were roughly twice as fast to deliver, with average total delivery times of 4.1±0.7 min compared with 8.2±2.6 min for the MLC plans.
Design details
The team also examined the effect of various compensator design parameters on plan quality. First, they varied the compensator resolution from 2 to 10 mm for the five head-and-neck plans. While there was no clear trend in OAR doses, PTV coverage was inferior at resolutions of 6-10 mm. PTV dose distribution was more homogeneous for finer resolutions.
They also assessed the effect of varying the maximum compensator thickness between 0.5 and 3.0 TVL (tenth-value-layer, which for tungsten is 2.14 cm) for two plans. In both cases, PTV doses were unaffected by maximum thickness, while OAR doses decreased as thickness increased. At 2 TVL, OAR sparing was similar to 6MV-MLC plans. The authors note that there is little benefit to using greater than 2 TVL and that 1.5 TVL may be acceptable.
Examining the source-to-compensator distance (SCD) revealed no clinical difference in plan quality between SCDs of 63 and 53 cm. Likewise, varying the number of beams from five to 13 did not reveal any clear trends in tumour or OAR dose. The team suggests that seven or nine beams would usually be appropriate.
The authors concluded that the compensator can deliver plans of comparable quality to MLC-based systems, even for 60Co beams. This makes the system well-suited to large portions of LMICs where 60Co units are the only available technology. They note that the compensator-ring system will also work as an add-on to a linac.
The team is now developing a prototype compensator system. “We have completed our initial round of planning studies, which has been very helpful in informing the design,” Ford told Physics World. “Together with our commercial partner in India under the NCI grant, we are pursuing a prototype and are about six months away from having something ready to test.”



