Surgical resection of cancerous tissue is a common treatment used to reduce the likelihood of cancer spreading to healthy tissues. However, the efficacy of such surgery strongly depends on the surgeon’s ability to distinguish between cancerous and healthy tissue.
It is known that the metabolic activities of cancerous and healthy tissue differ significantly: cancerous tissues often have chaotic blood flow combined with low levels of oxygen, or hypoxia. With hypoxic regions common in cancerous tissue, accurate identification of hypoxia could help to differentiate cancerous from healthy tissue during surgery.
Researchers from the Thayer School of Engineering at Dartmouth and the University of Wisconsin-Madison are investigating the use of fluorescent probes for real-time imaging of local oxygen concentration in tissue during surgery. They present their findings in the Journal of Biomedical Optics.
When fluorescent probes are excited by light, they return to the ground state and emit light at a different energy. Immediately upon illumination, probes emit a short optical light pulse known as prompt fluorescence. Some probes can also produce a delayed fluorescence signal some time after illumination.
Although both prompt and delayed fluorescence signals decay over time, the prompt fluorescence signal decays rapidly in comparison with the prolonged decay of delayed fluorescence. The delayed fluorescence signal decay can be observed and analysed further to better understand the metabolic activity of nearby tissue.
Real-time oxygenation assessment
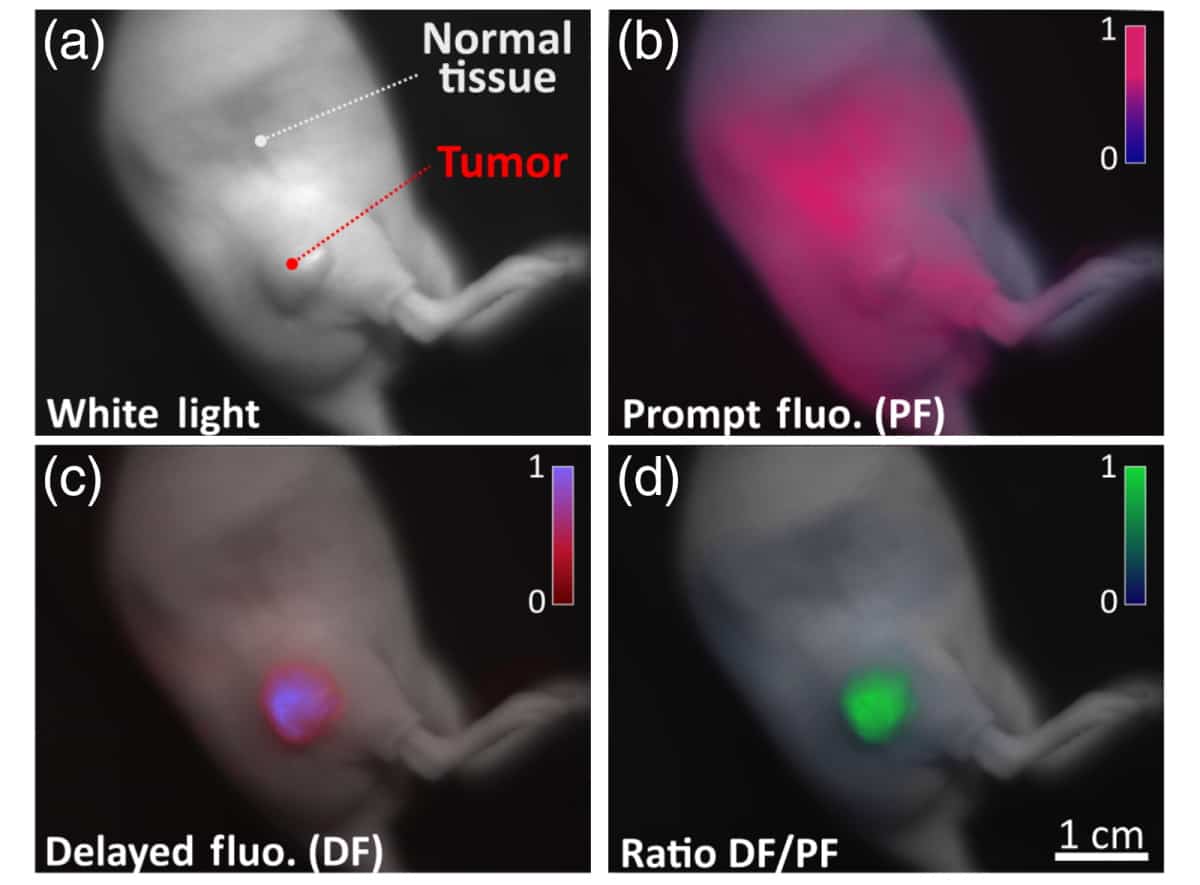
First author Arthur Petusseau and colleagues utilized an optical imaging system to monitor light emitted by the endogenous molecular probe protoporphyrin IX (PpIX) in a mouse model of pancreatic cancer where hypoxic regions are present.

The researchers administered the PpIX as either a topological ointment or via injection to the animal’s side flank and generated fluorescence using a 635 nm modulated laser diode as the excitation source. They found that the ratio of delayed to prompt fluorescence was inversely proportional to the local oxygen partial pressure in tissue.
The weak intensity of the delayed fluorescence signal makes it technically challenging to detect. To overcome this, the researchers utilized a time-gated imaging system that enables sequential monitoring of the fluorescence signal within small time windows only. This enabled them to reduce the detection of background noise and accurately monitor changes in the delayed fluorescence signal.
Further analysis showed that the delayed fluorescence signal acquired from cancerous hypoxic cells was five-fold greater than that obtained from healthy, well-oxygenated tissue. In addition, the team also found that the delayed fluorescence signal could be amplified further by tissue palpation (applying pressure to the skin during physical examination), which enhances the transient hypoxia and enables temporal contrast between the two signals.
“Because most tumours have micro regional hypoxia present, imaging hypoxia signals from PpIX delayed fluorescence allows for excellent contrast between normal tissue and tumours,” says Petusseau.
Multimodal spectroscopy detects brain tumours in vivo
The researchers conclude that monitoring delayed fluorescence arising due to the unique emissions of the PpIX fluorescent probe in the presence of hypoxia has several benefits in distinguishing between healthy and cancerous tissue during surgery. “Acquiring both prompt and delayed fluorescence in a rapid sequential cycle allowed for imaging oxygen levels in a way that was independent of the PpIX concentration,” they say.
“The simple technology required, and the fast frame rate capability coupled with the low toxicity of PpIX make this mechanism for contrast translatable to humans. It could easily be used in the future as an intrinsic contrast mechanism for oncologic surgical guidance,” claims Petusseau.



