Patients with early-stage breast cancer often undergo breast-conserving surgery, which involves local excision of cancer with a surrounding margin of healthy tissue. The goal is to remove the entire tumour and minimal healthy tissue, but excision is primarily based on visual inspection and relies on the surgeon’s expertise. Roughly 20% of patients require a second surgery due to incomplete initial removal of cancerous tissue.
Improving the tumour margin assessment during the operation could reduce the number of repeat surgeries and associated health and financial costs. Other options available for intraoperative margin assessment include projection radiography and, more recently, volumetric micro-CT. But these X-ray imaging techniques cannot effectively differentiate between normal, abnormal benign and malignant fibrous tissues.
A team from the Thayer School of Engineering at Dartmouth and Dartmouth-Hitchcock Medical Center is now investigating whether optical imaging could help, reporting their findings in Physics in Medicine & Biology.
“We choose to investigate optical scatter imaging, because it is non-contact, provides rapid scanning and relies only on endogenous contrast in the tissue,” explains first author Samuel Streeter. “The fine patterns of light used by the technique probe only superficial layers of tissue, making the approach particularly well suited for analysing tissue margins.”
Optical scatter imaging
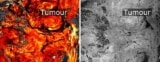
Streeter and colleagues used wide field-of-view optical scatter imaging to assess 57 resected breast tumour slices, containing 13 distinct tissue subtypes, from 57 patients. The optical scatter method employed, known as spatial frequency domain imaging, illuminates the tissue with one-dimensional sinusoidal light patterns and images the reflected light intensity. It rapidly images the top layer of tissue with increased sensitivity to tumour-associated, collagen-rich matrix structures.
For comparison, the researchers also imaged the samples with micro-CT and diffuse white light (DWL) imaging, which is similar to the surgeon’s view in the operating room. To enable quantitative comparison between the three modalities, they converted the colour DWL images to greyscale intensity (luminance) and derived monochromatic optical scatter images from the shortest wavelength (490 nm).

In general, the optical scatter images exhibited similar contrast to the micro-CT view of the tissue. The team quantified the similarity between the micro-CT and optical images using two image similarity metrics: mutual information (MI) and the Dice coefficient. For healthy and benign tissue specimens, both optical scatter and DWL images exhibited similar Dice coefficients and similar MI to micro-CT.
However, for the cancerous specimens, optical scatter imaging exhibited greater MI with micro-CT than DWL with micro-CT, as well as greater (for invasive ductal carcinoma) or similar (for invasive lobular carcinoma) Dice coefficients with micro-CT. Analysing all specimens together revealed that optical scatter images exhibited greater similarity with co-registered micro-CT in 89% of specimens using MI and in 81% using the Dice coefficient.
The researchers next analysed the coefficient-of-variation, a measure of the amount of feature content in each image, in all of the wide-field images. In all specimens, optical scatter imaging gave significantly higher values (representing the highest image quality) than either DWL or micro-CT, revealing additional features associated with fibrous tissue structures that may be of diagnostic relevance.
Finally, they analysed micro-CT, optical scatter and DWL images of 2.0 x 2.0 cm regions containing boundaries between malignant tissue and healthy or benign fibrous tissue. In four representative specimens, optical scatter exhibited the highest coefficient-of-variation and the highest contrast ratios across the boundaries, suggesting a greater sensitivity to malignant–fibrous tissue boundaries.
The researchers note that micro-CT is sensitive to microcalcifications, which are related to breast cancer histology and are not visible in the optical images. Along with the fact that micro-CT cannot clearly differentiate fibrous tissues, the optimal approach for margin assessment during breast cancer surgery may be to couple the two modalities.
Optical imaging checks tumour margins during breast cancer surgery
“This study focused on demonstrating the benefits of optical scatter imaging using tumour slices,” says Streeter. “But to truly combine these modalities in a clinical tool, the optical scatter imaging should be mapped to the three-dimensional surface of the specimen and not just constrained to flat tissue surfaces.”
As such, the team is now using established 3D optical imaging techniques to advance optical scatter imaging by mapping the reflectance to 3D structures. “In so doing, we will be able to overlay optical scatter reflectance from intact specimen margins with the volumetric micro-CT scan,” Streeter tells Physics World. “This multimodal solution could help clinicians identify suspicious margins rapidly – in the operating room – in order to avoid costly re-excision procedures.”



