Portable MRI (pMRI), a new type of very low-field MRI scanner that does not require dedicated shielding, can effectively diagnose stroke and detect blood clots in the brain as small as 4 mm in size. In a study of 50 patients with ischaemic stroke treated at Yale New Haven Hospital, intracranial imaging with pMRI detected ischaemic infarcts in 90% of patients. The prospective study, described in Science Advances, is the first to demonstrate that the 0.064 T Swoop portable MRI system can be used to definitively diagnose and assess stroke at a patient’s bedside.
The ability to rapidly distinguish ischaemic stroke, where a blockage cuts off the blood supply to the brain, from haemorrhagic stroke, in which there is bleeding in the brain, is critical to expedite effective clinical treatment. Ischaemic stroke, the most common type of stroke, is usually treated with thrombolytic “clot busting” treatment. This approach, however, is not appropriate for haemorrhagic strokes.
As such, both the European Society for Cardiology and American Heart Association advise that all stroke patients receive rapid brain imaging on hospital arrival to rule out intracranial haemorrhage. CT is the imaging method of choice for diagnosing haemorrhagic stroke, with radiation-free MRI becoming increasingly popular; but access to stationary MRI machines can be limited.

Low-field pMRI scanners could prove the ideal approach for point-of-care diagnosis. The Swoop pMRI scanner, which incorporates an eight-channel radiofrequency head coil, operates from a standard electrical outlet, does not require cryogenics and integrates electromagnetic interference rejection, removing the need for a shielded room.
Its compact size (140 cm high and 86 cm wide) enables use in inpatient or emergency department settings, and it does not require a specialized MRI technician for operation. Importantly, the pMRI is not affected by and does not compromise the functionality of nearby hospital equipment.
“A mobile, bedside solution for portable MRI-based imaging opens the doors for re-imagining how we can deliver high-quality care, reach patients and communities across the globe, and further understand the basis for neurological injury and health,” says principal investigator Kevin Sheth from Yale School of Medicine.
For the study, the researchers used low-field pMRI to perform bedside intracranial imaging for 50 patients with ischaemic stroke. The pMRI scans were performed an average of 37±60 hr after the patient’s last known normal time (unknown for five patients). Six patients underwent pMRI in the emergency department, 40 in a neuroscience intensive care unit (ICU) and four in a COVID-19 ICU.
The team acquired a total of 50 T2-weighted, 51 fluid-attenuated inversion recovery (FLAIR) and 56 diffusion-weighted imaging (DWI) images, with a mean exam time of about 25 min. Each of the 50 patients had an ischaemic infarct detected by standard-of-care neuroimaging – high-field MRI or non-contrast CT – within 36 hours of the pMRI exam.
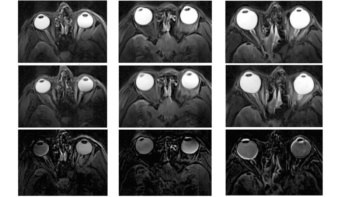
Sheth and colleagues evaluated and compared each low-field pMRI with the conventional MRI or CT scan acquired closest to the time of the pMRI exam. The pMRI was considered to have correctly detected an ischaemic infarct (which appeared as a hyperintense region) if at least one sequence showed the same infarct as seen on the standard exam.
The pMRI detected infarcts in 45 patients across cortical, subcortical and cerebellar structures. The researchers report that “stroke volume measurements were consistent across pMRI structural sequences and pMRI measurements were in agreement with conventional MRI measurements”. They also note that pMRI stroke volumes significantly correlated with stroke severity at the time of exam and functional outcome at patient discharge.
Sheth believes that the team’s results are just the beginning for pMRI. “Hardware and software improvements, algorithm development and image quality improvements, and the science of interpretation and utility must be developed urgently in order to unlock the potential of this approach,” he tells Physics World. “That development needs careful validation from the clinical and scientific community.”
“We’ve seen progressive improvement in imaging resolution and scan times, which will expand access to timely neuroimaging,” adds co-author W Taylor Kimberly from Massachusetts General Hospital. “Due to the portability, this technology can be considered for a variety of scenarios where MR imaging was not previously available. We’re looking forward to continuing to advance the clinical application and validate its use for stroke.”
Portable brain MRI scanner increases access to neuroimaging

Writing in an accompanying commentary, Peter Basser from the National Institutes of Health describes pMRI as a milestone in medical imaging. “Owing to their reduced cost and portability, these scanners could be deployed in a myriad of new settings, such as sporting events or rock concerts, rural health care centres, emergency rooms and assisted living facilities,” he writes.
Basser notes that the portability and ease-of-use of this type of device could make medical imaging more widely available in resource-limited environments. “If urgent care facilities or local hospital emergency rooms offered portable low-field brain MRI as readily as they offer ultrasound imaging, for instance, then it would help bridge this gap in patient access to emergency medical care,” he explains. “Overall, deploying portable, low-cost and easy-to-use brain imaging systems could democratize the delivery of critical medical imaging services and resources.”