Delivering whole-brain radiotherapy in a single, ultrafast dose minimizes the cognitive impairment associated with damage to the hippocampus. This, at least, is the case for mice, whose performance in a series of object-recognition tests was measured after whole-brain irradiation administered in either one sub-second dose or extended over a conventional four-minute duration. The effect is due to the smaller inflammatory response provoked by more rapid treatments compared with conventional dose rates, and could one day lead to radiation therapies with reduced side effects.
It is easy to see the appeal of administering an entire course of radiotherapy in a single dose. Apart from being more convenient for the patient, ultra-rapid irradiation means that the effect of patient motion can be virtually disregarded. When dose delivery is near-instantaneous, even moving targets appear practically stationary. But even without these advantages, the technique – named “FLASH” in an in vitro study from 2014 – has intrinsic radiobiological benefits that are only just coming to prominence.
“Certain aspects of FLASH radiobiology have been discovered and rediscovered since the 1960s,” says Billy W Loo Jr of Stanford University School of Medicine, who conducted this latest research with a team from the departments of radiation oncology and neurology & neurological sciences. “The 2014 study was the first to gain general recognition, and even then it was slow, in part because it didn’t fit with accepted radiobiology paradigms, and also because people could not see a practical path to clinical implementation.”
That path has become clearer now that Loo and colleagues have started development of a linac that can deliver the high dose rates necessary to implement FLASH clinically. This has prompted more work on the radiobiological aspect of the technique, leading to the promising results reported by Loo and his team in this latest study (Radiother. Oncol. 10.1016/j.radonc.2019.06.006).
The researchers divided healthy mice into three groups. One group underwent a whole-brain electron radiotherapy procedure delivered at the standard dose rate; one group received the same overall dose but in a single fraction lasting less than a fifth of a second; a control group received no treatment at all.
Ten weeks after the treatments, the researchers observed the mice responding to unfamiliar objects placed within and moved around a testing environment. Mice in the control group and the FLASH group spent about the same time investigating these changes to their environment, whereas mice that had received the standard irradiation procedure appeared significantly less sensitive.
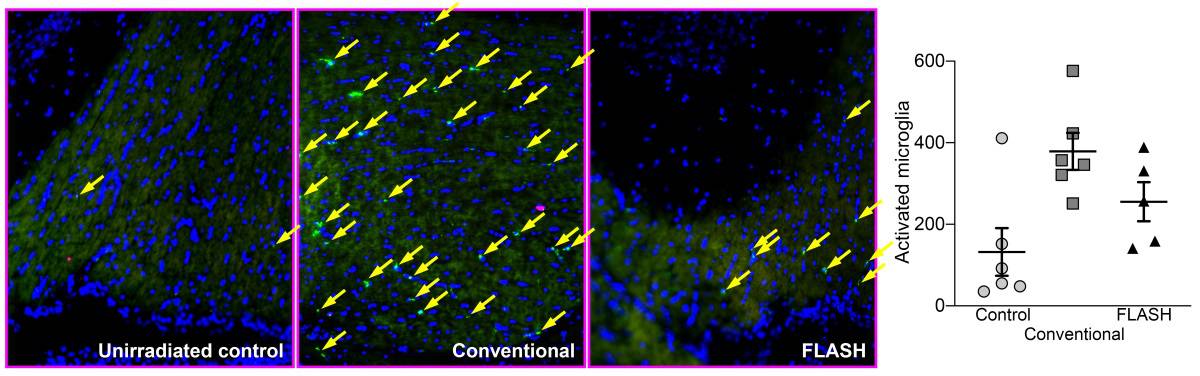
When the mice were sacrificed and their brains analysed, Loo and colleagues found two major differences linked to the groups’ varying cognitive performance. The first was an indication of inflammatory response, expressed by the presence of activated microglia and cytokines, especially in the conventional-dose-rate group. In the FLASH group, these indicators of brain damage appeared at a level intermediate between the control and the conventional-irradiation groups.
The second difference was seen in the density of dendritic spines in the mice’s hippocampi. These subcellular structures help pass signals between neurons, and play a role in memory formation. Spine density in the conventional-irradiation group was much lower than that seen in the control group but was largely preserved in the mice that underwent FLASH.
“There is evidence that the anatomic and functional changes are a result of the neuroinflammation,” says Loo. “So at one level, the mechanism of FLASH sparing of brain injury appears to be through reduced neuroinflammation compared to conventional-speed irradiation.”
PHASER linac will translate FLASH radiotherapy to the clinic
Why the same radiation dose delivered at a much higher rate should have such an effect is not clear, however. “Ultimately, this is still a phenomenological observation. We need to do more work to understand specifically why FLASH triggers less neuroinflammation,” says Loo.
Whatever the mechanism, human patients will not be benefiting from whole-brain FLASH for some time. Until the technology behind the group’s dedicated FLASH platform matures, the technique will be limited in the near term to superficial tumours using electron beams, or very small embedded tumours using narrow, single-angle proton beams.



